How big is the effect? What are the side
effects? How is suicide risk affected?
Chapter 7 in Brinkmann S, Petersen A
(eds.). Diagnoses: perspectives, criticism and discussion. Aarhus:
The authors and Klim; 2015 translated from Danish:
(Kapitel 7 i
Brinkmann S, Petersen A (red.). Diagnoser: perspektiver, kritik og
diskussion. Aarhus: Forfatterne og Klim; 2015):
http://www.deadlymedicines.dk/overdiagnostik-og-overbehandling-i-psykiatrien/
OVERDIAGNOSTIC AND OVERTREATMENT IN PSYCHIATRY translated from Danish: (OVERDIAGNOSTIK OG OVERBEHANDLING I PSYKIATRIEN:) http://www.deadlymedicines.dk/wp-content/uploads/2015/09/Diagnoser_kap-7.pdf
Page 168:
Do antidepressants have any effect on
depression?
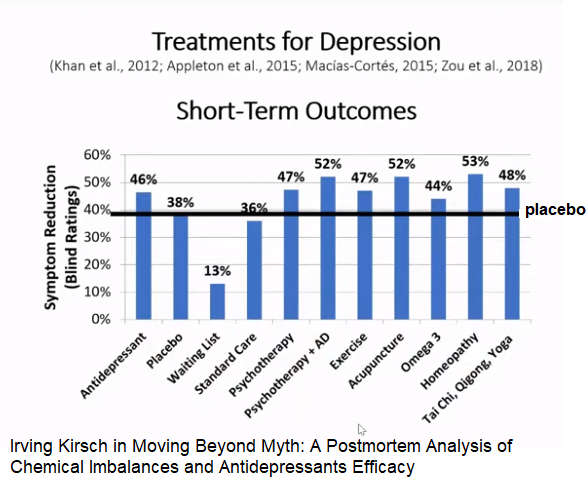
In round numbers, the randomized trials show that
around 50%
of patients get better on an antidepressant and 40% on
a placebo.
The effect in the 40% is often called a placebo effect,
but it is
does not. Many of the patients would have gotten better,
even if you didn't
had given them any treatment at all, as most
depressions
goes away on its own after a few weeks. When both
doctors and patients “have
experience for" that the
treatment works, we must therefore say that we cannot
use that
"experience" for something, since we don't know how it
would be
gone without treatment.
The difference of 10% means
that only one patient benefits
of treatment when treating ten
patients. The real effect is
however, much less, if it exists at
all. The experiments have
namely not been properly blinded.
Antidepressant drugs have significant
side effects, and many
patients and their doctors therefore want to know about it
blinded
drug contains active substance or placebo. A systematic
review of
21 trials in a number of different diseases that had
both a
blinded and an unblinded observer, found that the treatment
effect
was overestimated by 36% on average (measured as odds
ratio),
when the unblinded observer assessed the effect
(Hróbjartsson et al.
2012). Most trials had used subjective
effect measures, and the effect
of antidepressants is also
assessed on very subjective scales (e.g. the Hamilton scale).
If
we assume that the blinding is broken for all the patients
in the
trials with antidepressants, and adjusts for the overestimation of
the effect,
the loss of blinding causes, we find that
antidepressants do not have
no effect (odds ratio 1.02) (Gøtzsche
2015a).
The blinding is probably not broken for all the patients,
but you only have to
misclassify 5% of patients as to whether they
have had an effect or
not until the apparent effect of
antidepressants disappears (since 50%
with effect on active
substance becomes 45%, and 40% on placebo also becomes 45%)
Page
177:
Brain damage
The situation is that the medication keeps
the patients stuck in the patient role
and changes their
personality (Gøtzsche 2015a; Healy 2004; Kessing
et al. 2005;
Whitaker 2013), so they don't learn to deal with life's
challenges.
Unfortunately, the opinion of leading psychiatrists is
exactly the opposite.
They say it is important to take
antipsychotics and antidepressants because
untreated schizophrenia
(Lægemiddelindustriforeningen 2013) and depression
(Videbech &
Dalsgaard 2014) can cause brain damage. I consider this
for being
an equally unpleasant example of abuse of power, misinformation
and
persuasion as the rock of the chemical imbalance.
Drag Info Madinamerica.com: Antidepressants as a treatment for depression https://www.madinamerica.com/drug-info-antidepressants/
Irving Kirsch et al. 2002: The Emperor's New Drugs: An Analysis of Antidepressant Medication Data Submitted to the U.S. Food and Drug Administration. “The proportion of the drug response duplicated by placebo was significantly greater with observed cases (OC) data than with last observation carried forward (LOCF) data. If drug and placebo effects are additive, the pharmacological effects of antidepressants are clinically negligible.”
Jeffrey R. Vittengl 2017: Poorer Long-Term Outcomes among Persons with Major Depressive Disorder Treated with Medication. “The presence of major depressive disorder (MDD) and receipt of mental health treatment predicted greater depressive symptoms 9 years later”. The FDA’s “Major Depressive Disorder: Developing Drugs for Treatment Guidance for Industry” states the following: “Antidepressants in established classes (e.g., SSRIs, SNRIs) typically need studies of 6 to 8 weeks duration to demonstrate efficacy.”
Hengartner M.P · Angst J.· Rössler W.2018: Antidepressant Use Prospectively Relates to a Poorer Long-Term Outcome of Depression: Results from a Prospective Community Cohort Study over 30 Years. https://www.karger.com/Article/Abstract/488802
Hengartner et al. 2019:
‘Newer-generation
antidepressants and suicide risk in randomized controlled trials: A
re-analysis of the FDA database’
New
study: antidepressants significantly raise the risk of suicide in the
treatment of depression for adults:
“Earlier analysis of
this data did not reveal the increased risk because the method used
was incorrect.
Previously, calculations were based on ‘person
exposure years’ (PEY) rather than the number of patients receiving
treatment...
Suicide attempts and suicides combined was about 2.5
times higher”.
“Our findings thus conflict with the work by
Khan et al. [5], who based their effect estimates on PEY rather than
the number of patients.
When hazards are not constant over time,
PEY is inappropriate [10] and may obscure a true adverse drug effect”
Hengartner et al. 2019: Reply to the Letter to the Editor: “Newer-Generation Antidepressants and Suicide Risk: Thoughts on Hengartner and Plöderl’s Re-Analysis”: To demonstrate that misreported suicides can substantially bias the results, we show in Table 1 that the suicide risk accord-ing to a Bayesian random-effects meta-analysis (the method rec-ommended by Ren et al. [6]) of the uncorrected data table was OR = 2.49, 0.82–45.32 (note the discrepancy to Hayes et al. [1]).
Ny studie sår fornyet tvil om medisiner mot depresjon
Forskningen på antidepressiva har
så store metodeproblemer at vi ikke kan stole på resultatene,
ifølge en ny analyse. Anerkjent professor er uenig.
Systematisk
skjevhet, utvalg av positive resultater, mangelfull rapportering av
bivirkninger. Det er noen av problemene i studiene av medisiner mot
depresjon.
Metodeproblemene er så store at vi ikke vet om
medisinene
virker.
https://forskning.no/angst-depresjon-medisiner/ny-studie-sar-fornyet-tvil-om-medisiner-mot-depresjon/1359079
How common and severe are six
withdrawal effects from, and addiction to, antidepressants? The
experiences of a large international sample of patients
Author
JohnRead https://doi.org/10.1016/j.addbeh.2019.106157
•Over half (55%) of people who had
tried to come off or reduce antidepressants report some degree of
difficulty coming off, with 27% ticking ‘very difficult’
•61%
report ‘withdrawal effects’, with 44% of these describing the
effects as ‘severe’
•40% report ‘addiction’, with 39% of
these describing their addiction as ‘severe’
•‘Anxiety/panic’
(66%) and ‘Irritability (62%) are particularly common.
•Less
than 1% had been told anything about withdrawal effects or
dependence.
https://www.sciencedirect.com/science/article/abs/pii/S0306460319309001?via%3Dihub
Forskere konkluderer: «Lykkepiller»
virker ikke mot depresjon
Stor gjennomgang av forskning tyder på
at SSRI-medisiner mot depresjon gjør mer skade enn nytte. Men
hvorfor opplever da noen at de hjelper? Marie Barse JOURNALIST,
VIDENSKAB.DK PUBLISERT Lørdag 18. februar 2017 –
04:00
https://forskning.no/depresjon/forskere-konkluderer-lykkepiller-virker-ikke-mot-depresjon/364440
James Davies et al. 2019: Clinical
guidelines on antidepressant withdrawal urgently need
updating
Letters Antidepressant withdrawal
Clinical guidelines
on antidepressant withdrawal urgently need updating
BMJ 2019; 365
doi: https://doi.org/10.1136/bmj.l2238 (Published 20 May 2019)
Cite
this as: BMJ
2019;365:l2238
https://www.bmj.com/content/365/bmj.l2238utm_source=twitter&utm_medium=hootsuite&utm_term=&utm_content=&utm_campaign=editors
Susan McPherson et al. 2019:
Long-term outcomes of trials in the National Institute for Health and
Care Excellence depression guideline:
“The forthcoming National
Institute for Health and Care Excellence depression guideline reviews
short-term outcomes for long-term depression. We present effect sizes
for long-term outcomes in trials that report these data.
Psychological therapies become more effective, whereas
antidepressants become less effective over the long
term.”
https://www.researchgate.net/publication/335693982_Long-term_outcomes_of_trials_in_the_National_Institute_for_Health_and_Care_Excellence_depression_guideline
Campaigning forces Royal College of Psychiatrists to change its position on antidepressant withdrawal by CEP Admin on 30/05/2019
Ny studie sår fornyet tvil om
medisiner mot depresjon.
Forskningen på antidepressiva har så
store metodeproblemer at vi ikke kan stole på resultatene, ifølge
en ny analyse. Anerkjent professor er uenig.
Marie Barse
JOURNALIST, VIDENSKAB.DK PUBLISERT Fredag 19. juli 2019 –
04:30
https://forskning.no/angst-depresjon-medisiner/ny-studie-sar-fornyet-tvil-om-medisiner-mot-depresjon/1359079
Anti-depressants CAN ruin lives: Major U-turn as psychiatrists say millions of patients MUST be warned over severe side effects. By BEN SPENCER MEDICAL CORRESPONDENT FOR THE DAILY MAIL PUBLISHED: 22:00 BST, 29 May 2019
-For years side effects of withdrawing from antidepressants were branded 'mild'
-But the Royal College of Psychiatrists has now changed its position to 'severe'
-UK prescribes more antidepressants than any other Western country
Keller
et al. 2001 «Study
329» (Wikipedia)
der en re-analysis
av rådata korrigerte den opprinnelige
konklusjonen.
In conclusion, the findings of this (original) study
provide evidence of the efficacy and safety of Paxil in the treatment
of adolescent depression.
The reanalyses concluded that "[t]he
efficacy of paroxetine and imipramine was not statistically or
clinically significantly different from placebo for any prespecified
primary or secondary efficacy outcome," and that there were
"clinically significant increases in ... suicidal ideation and
behaviour and other serious adverse events in the paroxetine group
and cardiovascular problems in the imipramine group."
Maß, R,. Backhaus, K., Lohrer, K., Szelies, M., & Unkelbach, B. K. (2023). No benefit of antidepressants in inpatient treatment of depression. A longitudinal, quasi experimental field study. Psychopharmacology. https://doi.org/10.1007/s00213-023-06417-4
Winfried Rief, John M. Kelley, Yvonne Nestoriuc, (2023). Placebo and nocebo effects in depression: Implications for treatment and clinical trial designs. “ Although antidepressants show statistically greater efficacy compared to placebos, the effect sizes are small, and the specific effect of these drugs provides only a small clinical benefit to patients.Placebo responses in double-blind trials are about 80% as large as the response to antidepressants.” https://doi.org/10.1093/med/9780197645444.003.0016
Jahanna Moncrieff et al. 2022: The
serotonin theory of depression: a systematic umbrella review of the
evidence
The main areas of serotonin research provide no
consistent evidence of there being an association between serotonin
and depression, and no support for the hypothesis that depression is
caused by lowered serotonin activity or
concentrations.https://www.nature.com/articles/s41380-022-01661-0
Inner Compass Initiative. Strømmet direkte 1. sep. 2022: Moving Beyond Myth: A Postmortem Analysis of Chemical Imbalances and Antidepressants Efficacy. https://www.youtube.com/watch?v=5pGkjBnrPe8