The standardized mortality ratio or SMR, is a quantity, expressed as either a ratio quantifying the increase or decrease in mortality of a study cohort with respect to the general population.
Shockingly, over the last 5 years, a series of large studies, some looking at national databases, have shown that patients with psychosis are 2 to 3 times more likely to die in any one year than the rest of us. Death is primarily by heart attack or stroke. Being two or three times more likely to be dead may not sound much but other studies point to 15-20 years of lost life.
Patients with schizophrenia are 10 times more likely to be dead at the end of the first year of treatment than they were 100 years ago. There is no other illness in medicine where such a statement could be made.
See Healy et al (2012) Mortality in Schizophrenia.
Healy et al 2006: Lifetime suicide rates in treated schizophrenia: 1875-1924 and 1994-1998 cohorts compared. “RESULTS: The suicide rate in schizophrenia between 1875 and 1924 was 20 per 100 000 hospital years, a lifetime rate of less than 0.5%. The suicide rate for all psychoses was 16 per 100 000 hospital years. Current rates of suicide for schizophrenia and other psychoses appear 20-fold higher. CONCLUSIONS: These findings point to an increase in suicide rates for patients with schizophrenia.
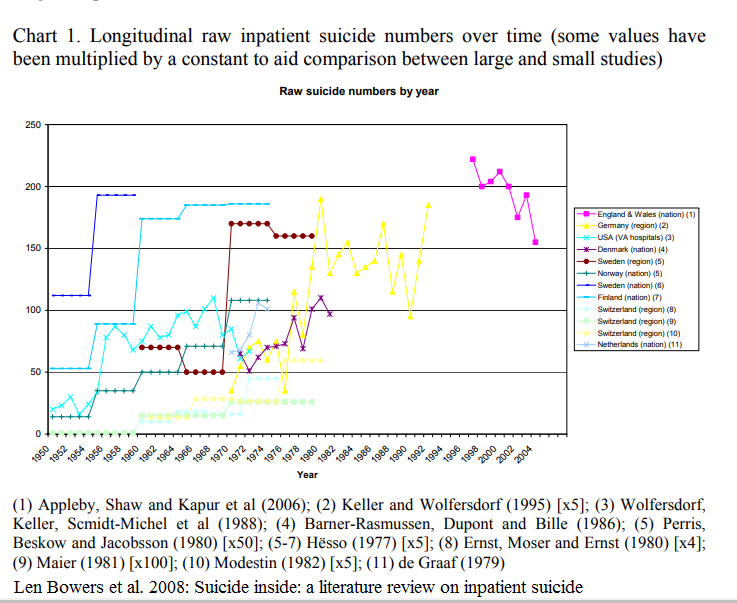
In the mid-50s antipsychotics / neuroleptics where introduced. In the 3 decades from 1950s to 1980s inpatient suicides in psychiatric hospitals ten doubled in Norway (Retterstøl 1988), raised from 50 to 400 per 100 000 in V.A. Hospitals ( Farberow 1975). Similar tendencies are reported from more that 8 countries (Chart 1: Bowers et al. 2008).
“SMRs for the 1970s, 1980s, and 1990s were 1.8, 3.0, and 3.2, respectively” (John McGrath et al. 2008) i.e. mortality rates continue to increase in several countries. “The most striking figure in this study is that eliminating suicide in schizophrenia would restore life expectancy to normal.” (David Healy et al 2012). Tiihonens 2009 FIN11 cohort study suggested that antipsychotic use decreased all-cause mortality. De Hert et al. 2010 showed incomplete reporting of data e. g. “A number of methodological and conceptual issues make the interpretation of these findings problematic, including incomplete reporting of data, questionable selection of drug groups and comparisons, important unmeasured risk factors, inadequate control for potentially confounding variables, exclusion of deaths occurring during hospitalization leading to exclusion of 64% of deaths on current antipsychotics from the analysis, and survivorship bias due to strong and systematic differences in illness duration across the treatment groups”.
Robert.Whitaker May 2020: Do Antipsychotics Protect Against Early Death? A Review of the Evidence. «In both psychiatric and non-psychiatric patients, the use of antipsychotics doubles the risk of death in comparison to patients who do not take the medications.»
Robert
Whitaker October 2020: Viewpoint: do antipsychotics protect
against early death? A critical view «These findings (Tiihonen)
stand in contrast to studies in non-psychiatric patients that have
found that antipsychotics, because of their adverse effects on
physical health, increase the risk of early death.»
The
“antipsychotics lengthen lives” research of Jari Tiihonen is
flawed in so many ways.
Dr. Jeff Rubin: Does “Antipsychotic” Treatment Reduce Risk of Death? «To my dismay, after studying the relevant research, I have found that the current psychiatric medical approach for addressing these types of concerns appear to be causing far more harm than good.» All av Jari Tiihonen studies are commented. «While they were hospitalized, they were almost certainly on the drugs, according to one team of researchers who had engaged in a similar study using the same data set, and many were hospitalized multiple times. What the researchers actually meant by labelling the group the “no antipsychotic group” were patients who didn’t take them each time they were released from the hospital.»
The Lancet november 2019. Correspondence: Michael P Hengartner, John Read, Joanna Moncrief: «Considering the contradictory evidence that exists, it is incorrect to claim that antipsychotics reduce mortality risk in people with psychotic disorders and we should remain mindful of the possibility that they might increase this risk.»
Weinman et al., 2009: There is some evidence that long-term exposure to antipsychotics increases mortality in schizophrenia. More rigorously designed, prospective studies are urgently needed.
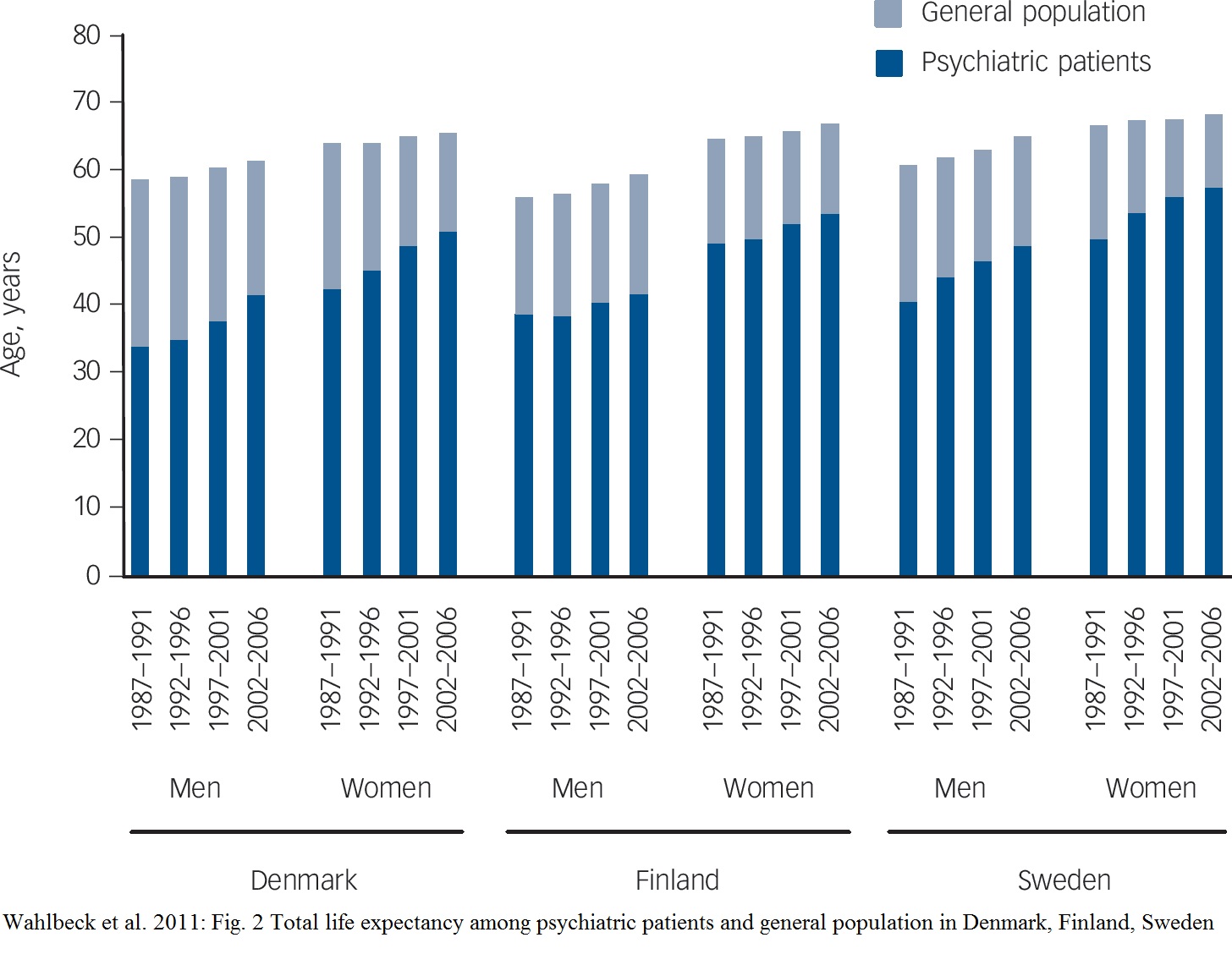
Reduced lifetime expectancy for male psychiatric patients in the 21st century was 22 years in Denmark, 19 years in Finland and 20 years in Sweden. This corresponded to the SMR for life expectancy of 2.5 for Denmark, 1.8 for Finland and 2.2 for Sweden, respectively. SMR for suicide was 25, 9 and 21, i.e. suicide is the dominant cause. Women's numbers are lower (Wahlbeck et al 2011).
(Norwegian) nationwide open cohort study from 2009 to 2015, including all Norwegians aged 20–79 with schizophrenia and/or substance use disorder registered in any specialized health care setting in Norway, a total of 125,744 individuals: SMR=11.6 for schizophrenia (Ina H. Heiberg et al. 2018).
“Thirty‐one participants (11%) were dead at follow‐up (SMR 11.56; 95% CI: 7.86‐16.42). Sixteen (6%) died by suicide (SMR 46.50, 95% CI: 26.58‐75.51); seven (2.5%) by accidental overdoses or other accidents, and eight (2.8%) from physical illnesses, including three (1%) from cardiovascular illness.” (Ingrid Melle et al. 2017)
“Cognitive behavioural therapy compared to treatment as usual reduced the risk of a new suicide attempt; risk ratio 0.47; 95% confidence interval 0.30–0.73; p = 0.0009; I2 = 57%.” (Peter C Gøtzsche et al. 2017)
In “Suicide in the Age of Prozac” Robert Whitaker focuses on the influence of antidepressants since the 90s.
However other studies mention neuroleptics. "Antipsychotics should be used more selectively, for shorter durations and with lowest possible effective dose." (Weinmann et al. 2010).
“People with serious mental illness die up to 20 years younger ...” … “Healthcare services should consider a shift away from physical health monitoring strategies and instead focus their resources on primary prevention strategies ... These include assertive smoking cessation (with pharmacological support), diet and exercise interventions and where possible, to avoid long-term prescription of antipsychotics associated with adverse metabolic outcomes.” (Athif Ilyas et al. 2017)
Literature/References:
Len Bowers,
Henk Nijman, Tumi Banda 2008. Suicide inside: a literature review on
inpatient suicide
https://www.kcl.ac.uk/ioppn/depts/hspr/archive/mhn/projects/litreview/LitRevSuicide.pdf
“Reported rates of inpatient suicide varied by all three
commonly used denominators – admissions, population and total
number of suicides – indicating that such figures are influenced
by social and service organisation factors. Rates in some countries
have risen during the latter half of the 20th Century. The reasons
for this are unknown”
Suicides in V.A: hospitals 1950 - 1974: http://wkeim.bplaced.net/files/antipsychotics-Figure-2-1024x768.gif (Farberow NL, Mac Kinnon D (1975) Status of suicide in the veterans administration. Report III ?)
Retterstøl N.
(1988) Increasing Suicide Rate in Scandinavian Psychiatric
Hospitals. In: Möller HJ., Schmidtke A., Welz R. (eds) Current
Issues of Suicidology. Springer, Berlin, Heidelberg. Suicides per
100000 patients per year in the psychiatric hospitals in Norway
increased from 35 in the period 1950-1954 to 373 in
1980-1984.
https://link.springer.com/chapter/10.1007/978-3-642-73358-1_12
Ina H. Heiberg et al. 2018. Total and cause-specific standardized mortality ratios in patients with schizophrenia and/or substance use disorder. “We performed a (Norwegian) nationwide open cohort study from 2009 to 2015, including all Norwegians aged 20–79 with schizophrenia and/or substance use disorder registered in any specialized health care setting in Norway, a total of 125,744 individuals. The SMRs were 4.9 (95% CI 4.7–5.1) for all schizophrenia patients, 4.4 (95% CI 4.2–4.6) in patients with schizophrenia without substance use disorder, 6.6 (95% CI 6.5–6.8) in patients with substance use disorder only, and 7.4 (95% CI 7.0–8.2) in patients with both schizophrenia and substance use disorder. ” https://journals.plos.org/plosone/article/file?id=10.1371/journal.pone.0202028&type=printable
Wahlbeck, K.,
Westman, J., Nordentoft, M., Gissler, M., & Laursen, T. (2011).
Outcomes of Nordic mental health systems: Life expectancy of
patients with mental disorders. British Journal of Psychiatry,
199(6), 453-458.
doi:10.1192/bjp.bp.110.085100
https://www.cambridge.org/core/journals/the-british-journal-of-psychiatry/article/outcomes-of-nordic-mental-health-systems-life-expectancy-of-patients-with-mental-disorders/D9769E301E9C238CA3B43E21E1913DF7
“Our results show that deinstitutionalisation can be
implemented while maintaining or even improving the life expectancy
of people with mental disorders across countries. In spite of the
transition of mental health services, however, the life expectancy
gap has remained largely unchanged over 20 years, and major health
inequalities persist between people with mental disorders and the
rest of the population.”
Psychiatry Ignores an Elephant in the Room By Peter Gøtzsche, MD September 21, 2017. https://www.madinamerica.com/2017/09/psychiatry-ignores-elephant-room/ “Large cohort studies of people with a first-episode psychosis provide a unique opportunity for finding out why so many young people with schizophrenia spectrum disorders die at a young age. However, it seems that those psychiatrists who have access to the mortality data generally do not want the facts to come out. In published cohort studies, there is virtually always too little information or no information at all about the causes of death.” Follow-up 16 February 2018, 8 March 2018, October 11, 2018 (Gøtzsche expelled from COCHRANE).
Ingrid Melle et al. 2017. Causes and predictors of premature death in first‐episode schizophrenia spectrum disorders. https://onlinelibrary.wiley.com/doi/full/10.1002/wps.20431 “Thirty‐one participants (11%) were dead at follow‐up (SMR 11.56; 95% CI: 7.86‐16.42). Sixteen (6%) died by suicide (SMR 46.50, 95% CI: 26.58‐75.51); seven (2.5%) by accidental overdoses or other accidents, and eight (2.8%) from physical illnesses, including three (1%) from cardiovascular illness.”
October 11, 2018 Mad in America. The Cochrane Collaboration Has Failed Us All. Robert Whitaker By Robert Whitaker: “There is now a scientific trail to follow in this exchange. The lead author of the TIPS study doesn’t respond to Gøtzsche’s inquiry (bad science); the editor of the journal that published the article won’t publish a letter raising the question about the deaths (bad science); and the research director for one of the funders doesn’t respond to the question either (more bad science). Instead, he writes a letter of complaint to Cochrane CEO Mark Wilson, stating that since Gøtzsche has a relationship with the Hearing Voices group, he isn’t going to believe anything that the Cochrane Collaboration publishes about mental illness!”
John McGrath et
al. 2008: Schizophrenia: A Concise Overview of Incidence,
Prevalence, and Mortality
https://academic.oup.com/epirev/article/30/1/67/621138
The SMRs for all-cause mortality significantly increased over
recent decades (p = 0.03): the median SMRs for the 1970s, 1980s, and
1990s were 1.8, 3.0, and 3.2, respectively.
Sukanta Saha et al. 2007: A Systematic Review of Mortality in Schizophrenia: The median SMR for those diagnosed in the 1970s, 1980s, and 1990s were 1.84, 2.98, and 3.20, respectively. The higher the SMR, the higher the rate of mortality.
Edward Chesney
et al. 2014: Risks of all-cause and suicide mortality in mental
disorders: a meta-review
https://onlinelibrary.wiley.com/doi/full/10.1002/wps.20128
The reduction in life expectancy associated with moderate to
heavy smoking ranged from 8 to 10 years. This range is similar to
that reported for a single depressive episode or recurrent
depressive disorder (7-11 years), but lower than that associated
with substance use (9-24 years), personality disorders (13-22
years), schizophrenia (10-0 years), and bipolar disorder (9-20
years) (Table 3).
Stefan
Weinmann, Volkmar Aderhold: Antipsychotic medication, mortality and
neurodegeneration: The need for more selective use and lower doses
February 2010(Psychosis) Psychological, Social and Integrative
Approaches 2(1):50-69
DOI: 10.1080/17522430903501999
https://www.researchgate.net/publication/233138682_Antipsychotic_medication_mortality_and_neurodegeneration_The_need_for_more_selective_use_and_lower_doses
"Antipsychotics should be used more selectively, for
shorter durations and with lowest possible effective dose."
Sukanta Saha et
al. Meta-analysis October 2007
A Systematic Review of Mortality
in Schizophrenia Is the Differential Mortality Gap Worsening Over
Time?
https://jamanetwork.com/journals/jamapsychiatry/fullarticle/210034
"With respect to mortality, a substantial gap exists
between the health of people with schizophrenia and the general
community. This differential mortality gap has worsened in recent
decades. In light of the potential for second-generation
antipsychotic medications to further adversely influence mortality
rates in the decades to come, optimizing the general health of
people with schizophrenia warrants urgent attention."
"People
with schizophrenia have a substantially increased risk of death
compared with the general population. Overall, people with
schizophrenia have 2.5 times the risk of dying. This review was able
to extract data from 37 studies that were conducted in 25 countries.
As predicted, the distribution of all-cause SMRs showed prominent
variability.
Confirming the hypothesis that the relative
mortality risk associated with schizophrenia is increasing, we found
that SMRs have increased in a linear fashion during the 3 decades
examined in this study. It is now widely acknowledged that
schizophrenia contributes substantially to the global burden of
disease. It is also well known that schizophrenia is associated with
elevated suicide rates."
Joukamaa M et
al. 2006: Schizophrenia, neuroleptic medication and mortality.
https://www.cambridge.org/core/journals/the-british-journal-of-psychiatry/article/schizophrenia-neuroleptic-medication-and-mortality/713F6B46E0A34BA1203761015F18684B
"The number of neuroleptics used at the time of the
baseline survey showed a graded relation to mortality. Adjusted for
age, gender, somatic diseases and other potential risk factors for
premature death, the relative risk was 2.50 (95% CI1.46–4.30) per
increment of one neuroleptic."
David Healy et
al 2012: Mortality in schizophrenia and related psychoses: data from
two cohorts, 1875–1924 and 1994–2010
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3488735/
"We found a 10-year survival probability of 75% in the
historical cohort and a 90% survival probability in the contemporary
cohort with a fourfold increase in standardised death rates in
schizophrenia and related psychoses in both historical and
contemporary periods. Suicide is the commonest cause of death in
schizophrenia in the contemporary period (SMR 35), while
tuberculosis was the commonest cause historically (SMR 9). In the
contemporary data, deaths from cardiovascular causes arise in the
elderly and deaths from suicide in the young.
The most striking
figure in this study is that eliminating suicide in schizophrenia
would restore life expectancy to normal."
Anne Høye et
al. 2011: Increasing mortality in schizophrenia: Are women at
particular risk? A follow-up of 1111 patients admitted during
1980–2006 in Northern Norway
https://helse-nord.no/Documents/SKDE/SKDE%20Artikler/Increasing%20mortality%20in%20schizophrenia,%20are%20women%20at%20particular%20risk%20(2011).pdf
"In Norway, mortality of patients with mental illness has
been reported
regularly since 1916 (Ødegård, 1936, 1951, 1952;
Ødegård, 1967;
Saugstad and Ødegård, 1979,1985; Hansen et
al., 1997). A previous
study based on the case register of the
University Hospital of North
Norway with follow-up 1980–1992
(Hansen et al., 2001) documented
increase in SMRs compared to
earlier periods, especially high for men...
Our study confirms
the persisting mortality gap between patients
with schizophrenia
and the general population over a period of 27 years,
with a
tendency of increasing SMRs."
Ilyas, A.,
Chesney, E., & Patel, R. (2017). Improving life expectancy in
people with serious mental illness: Should we place more emphasis on
primary prevention? The British Journal of Psychiatry, 211(4),
194-197. doi:10.1192/bjp.bp.117.203240
https://www.cambridge.org/core/journals/the-british-journal-of-psychiatry/article/improving-life-expectancy-in-people-with-serious-mental-illness-should-we-place-more-emphasis-on-primary-prevention/5BA82EA9FBBA0E932478CDC4AF6B4601/core-reader
“People with serious mental illness die up to 20 years younger
because of preventable physical disorders” … “Healthcare
services should consider a shift away from physical health
monitoring strategies and instead focus their resources on primary
prevention strategies that are provided to all people with serious
mental illness from the moment they first present to mental
healthcare services. These include assertive smoking cessation (with
pharmacological support), diet and exercise interventions and where
possible, to avoid long-term prescription of antipsychotics
associated with adverse metabolic outcomes.”
Dr. Jeff Rubin: Does “Antipsychotic” Treatment Reduce Risk of Death? «To my dismay, after studying the relevant research, I have found that the current psychiatric medical approach for addressing these types of concerns appear to be causing far more harm than good.»
Click on figure and table for enlargement:
.