{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}

[Norsk]
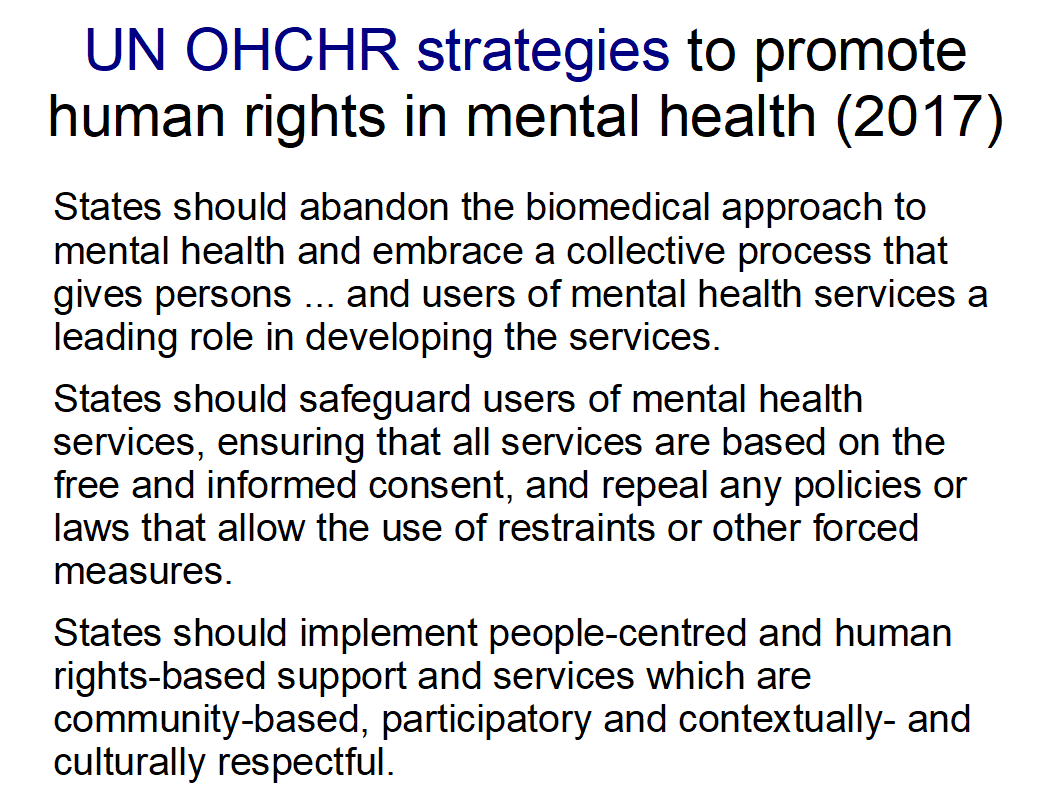
The United Nations Special Rapporteur on the right to health Mr. Pūras has 2017 called for «World needs “revolution” in mental health care». “There is now unequivocal evidence of the failures of a system that relies too heavily on the biomedical model of mental health services, including the front-line and excessive use of psychotropic medicines, and yet these models persist”
New WHO guidance seeks to put an end to human rights violations in mental health care, World Health Organization WHO 10. juni 2021
According to the guidelines, everyone diagnosed with psychosis must be offered neuroleptics. How many are medicated? What is the patient's reaction? How is the medication carried out? What could be the consequences of the cessation of coercion?
patient percentages medicated:
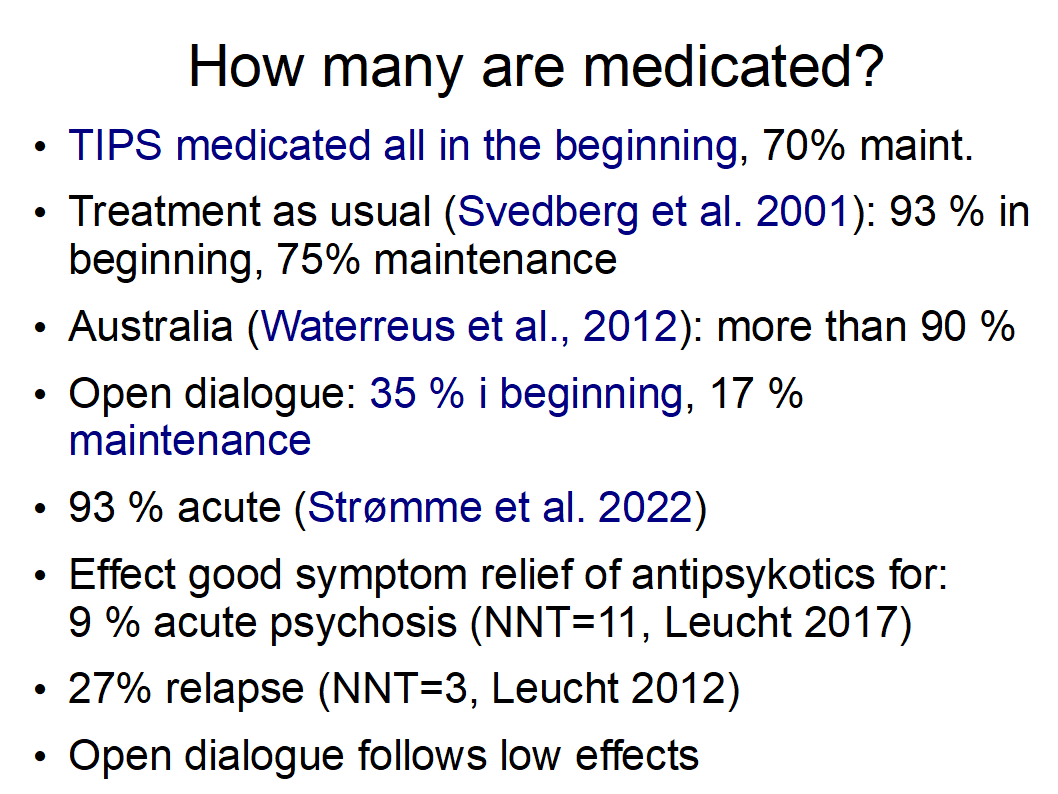
93% of all acute patients diagnosed with schizophrenia in the period 2014 to 2015 in Haukeland Hospital (Strømme et al. 2022): https://journals.lww.com/psychopharmacology/pages/articleviewer.aspx?year=2022&issue=01000&article=00007&type=Fulltext
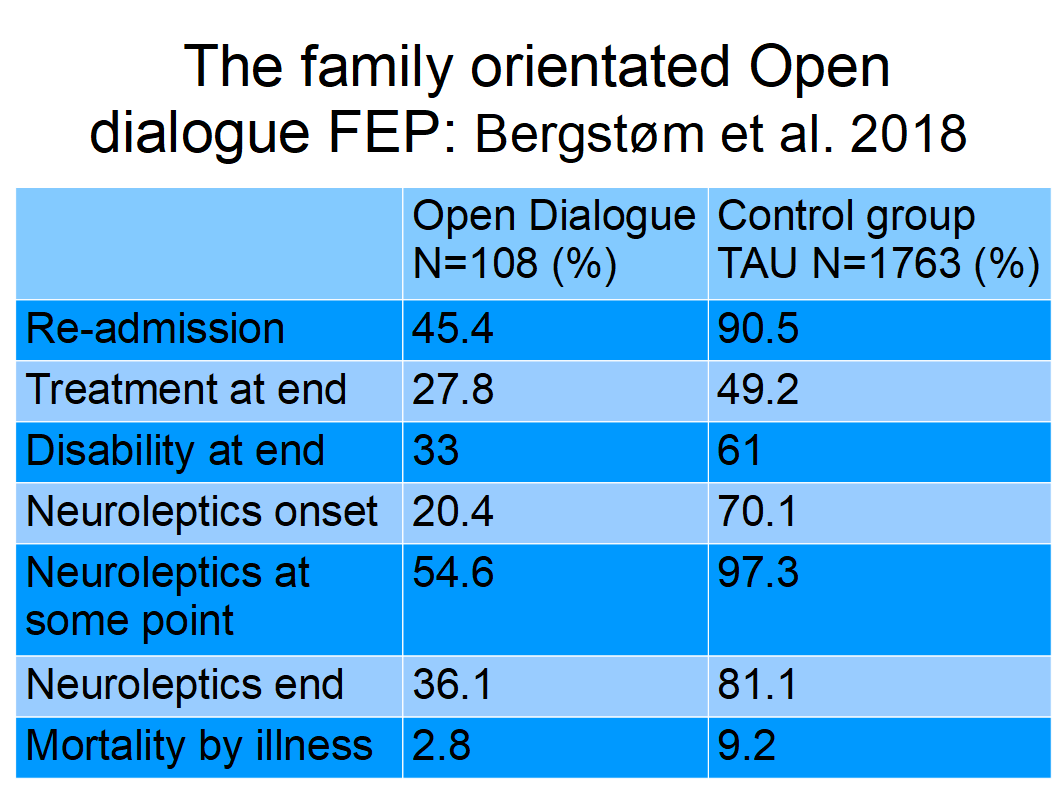
97,3% at one time or another with a diagnosis of psychosis in Finland: Bergstrøm et al. 2018: http://wkeim.bplaced.net/files/Bergstrom-2018.png
98%-100% of people diagnosed with schizophrenia inside our psychiatric units - and 90% living in the community - are on neuroleptics, The Guardian 2 March 2008: https://www.theguardian.com/commentisfree/2008/mar/02/mythoftheantipsychotic
The majority (91.6%) of participants diagnosed psychosis were using psychotropic medication (Waterreus et al. 2012)
93% of patients diagnosed with psychosis in Stockholm received antipsychotics (Svedberg et al. 2001)
96% of inmates diagnosed with psychosis medicated (Bjerkan og Bjørngaard 2011): https://www.dagensmedisin.no/artikler/2019/12/05/tvangsbegrensningsloven-har-et-hovedproblem/
99,5% inpatient services in Norway for the diagnosis of psychosis BBC February 2021: https://wso.no/wp-content/uploads/2021/02/BBC-radio-comment-English-translation.pdf
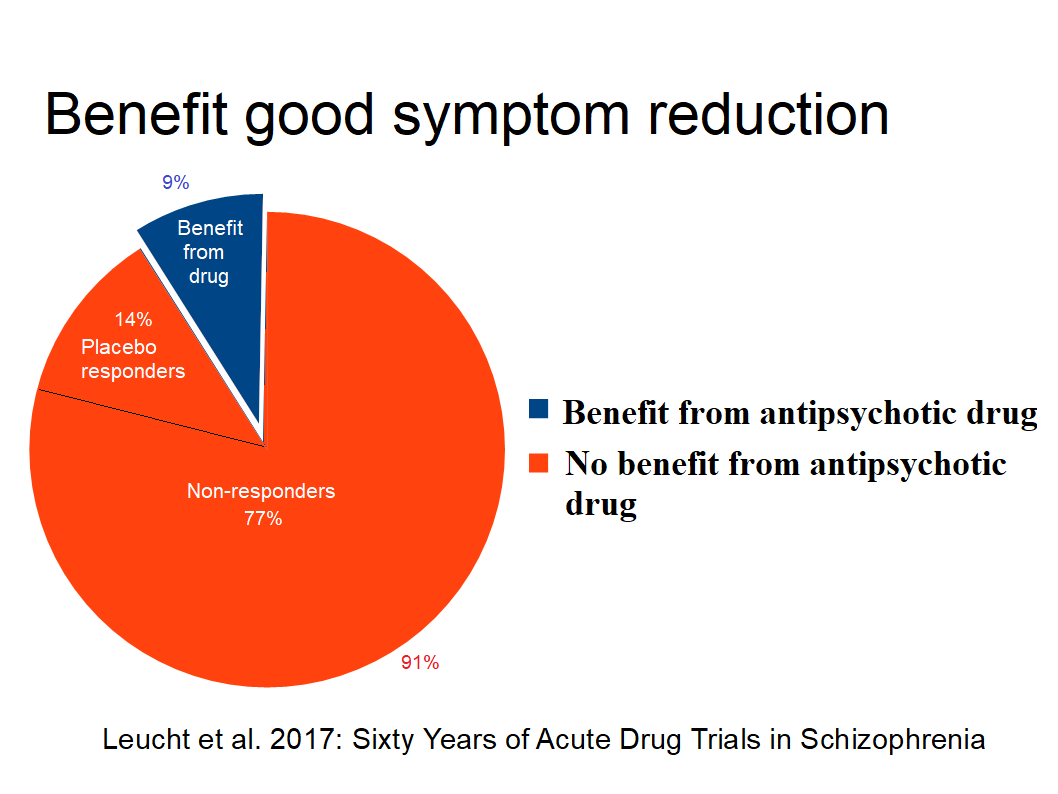
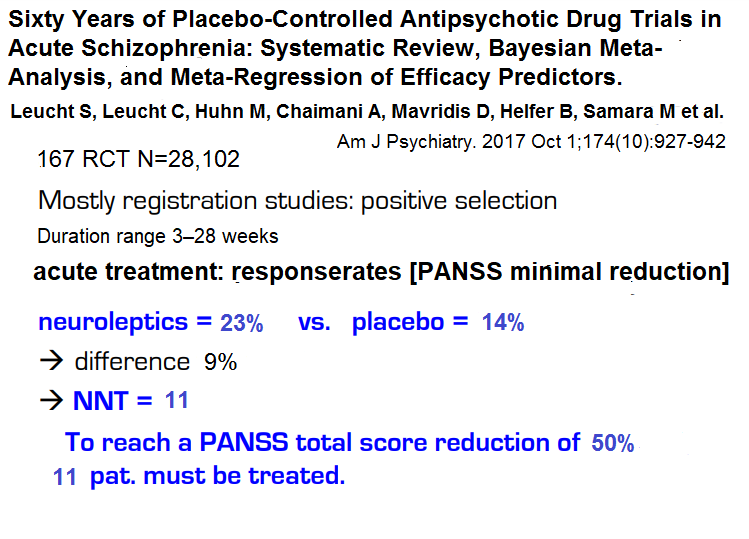
Double-blind studies of modern antipsychotics suggest that as many as 91 per cent of schizophrenia patients are without a genuine positive effect, i.e. good acute symptom reduction of the active substances (Leucht et al, 2017). It suggests that many non-responders receive antipsychotic treatment under pressure or coercion, and it is perhaps not surprising if some of them commit to change. These patients only experience side effects and inconvenience without benefit. It is professionally irresponsible.
Contents
How many are medicated with antipsychotics? Why and how is it done?
Lack of evidence for overmedication
Psychological interventions significantly superior to treatment as usual (TAU)
Forced medication
Tapering medication
The possibilities of the paradigm shift
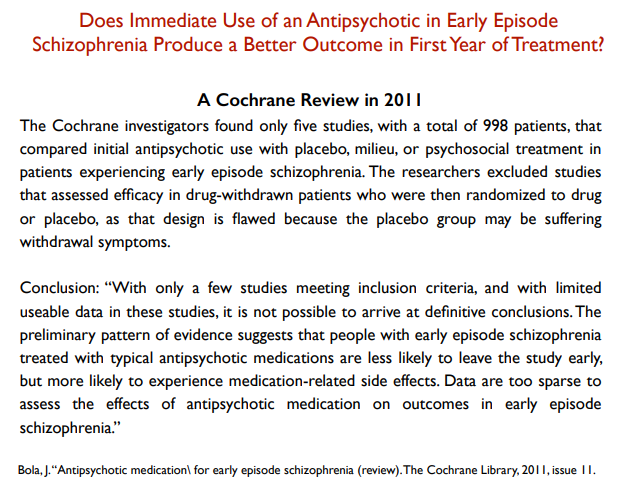
Because of. lack of studies of antipsychotic-naïve patients, the effect is uncertain. The Institute of Public Health concludes in 2019 in the Effectiveness of treatment for persons with psychosis:: "It is uncertain if antipsychotics compared to placebo affects symptoms in persons with early psychosis because we have very little confidence in this result." Bola 2011 and FHI 2021 ISBN 978-82-8406-251-8: The effect of antipsychotics on first episode psychosis reach the same result.
Danborg et al. 14 September 2019: «Benefits and harms of antipsychotic drugs in drug-naïve patients with psychosis: A systematic review» konkluderer: «The use of antipsychotics cannot be justified based on the evidence we currently have.»
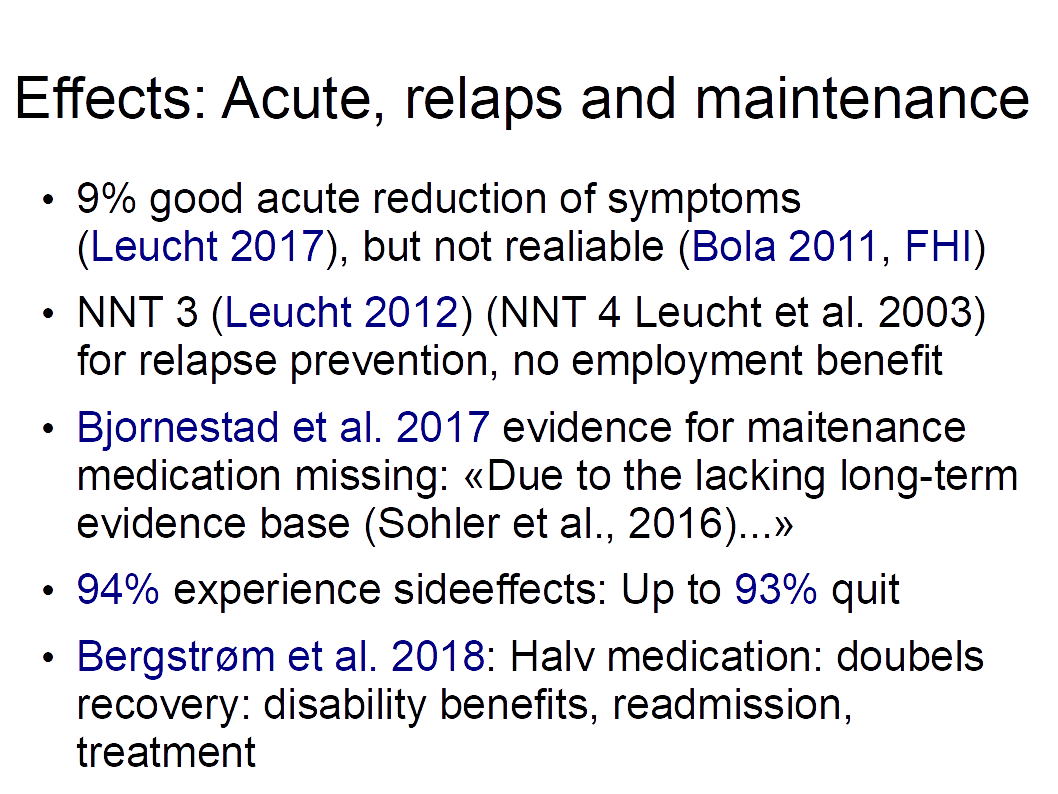
Good acute symptom reduction has a pharmaceutical effect for 9% of patients (Leucht et al. 2017), but the effect is uncertain as antipsychotic-naïve patients are missing. There is no evidence for long-term medication beyond 3 years (Sohler et al. 2015). Little uncertain effect and the fact that 94% (sources) experience side effects lead to "up to 93%" stopping neuroleptics.
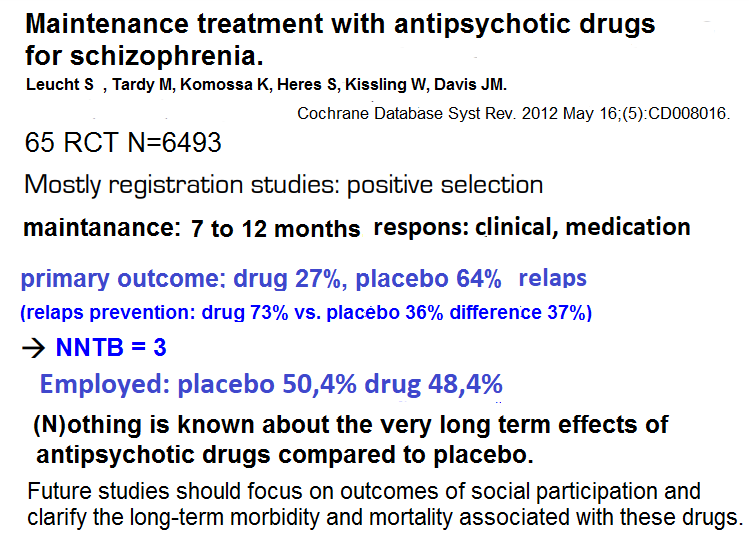
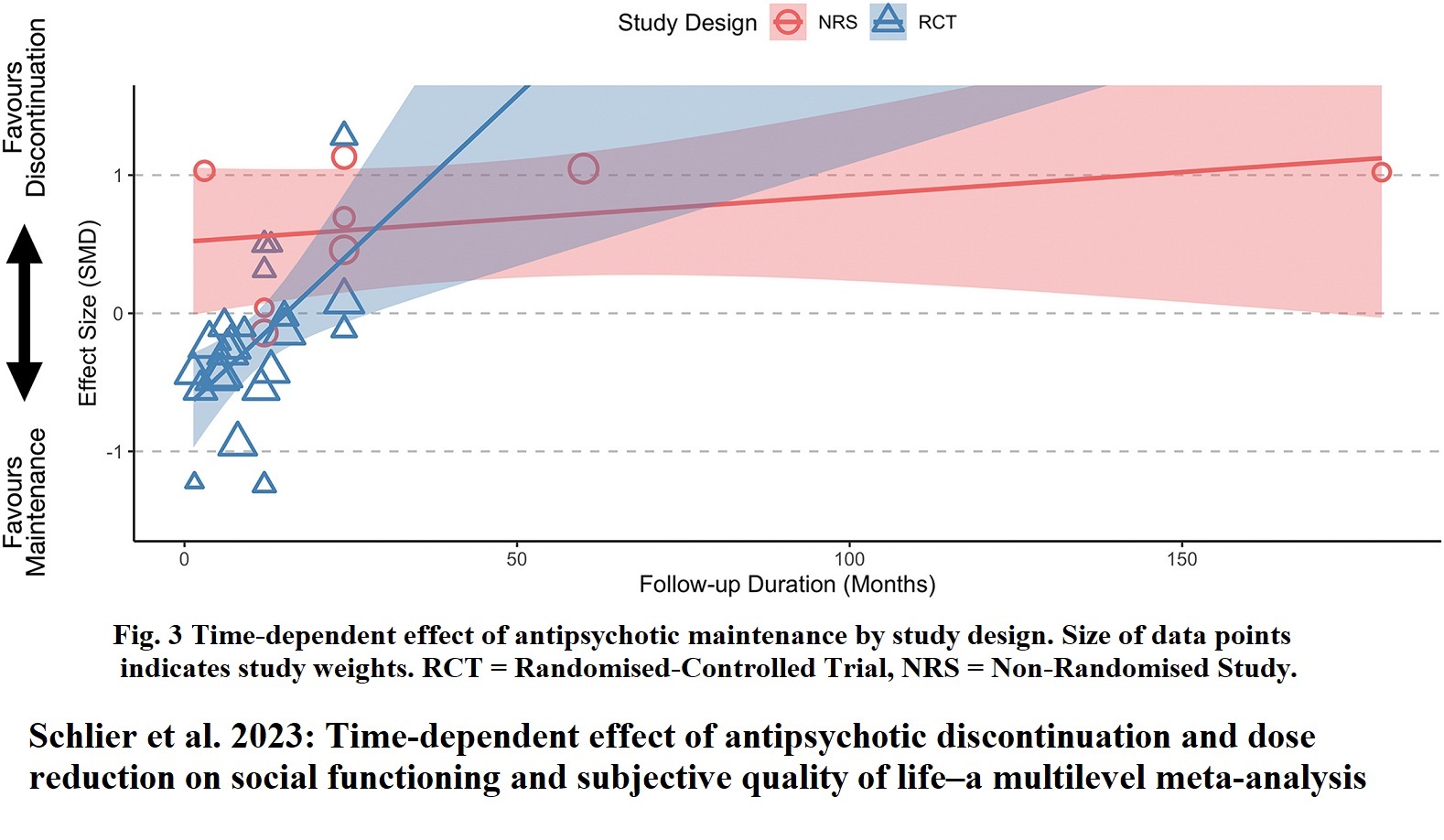
Leucht et al. 2012 with a length of 7 to 12 months is taken as income for maintenance effect with Number-Needed-to-Treat (NNT 3). but "(N)othing is known about the very long effects of antipsychotics compared to placebo" is not taken into account. It is claimed that maintenance medication protects against relapse, but the effect is time-dependent according to Ceraso, Leucht et al. 2020, see fig. 10. Schlier et al. 2023 conducted the first meta-analysis pooling the long-term effects of antipsychotic maintenance versus discontinuation on functional recovery in people with schizophrenia spectrum disorders. The result was that the benefit of maintenance disappears after two years. The clinical experience that the disease returns on discontinuation is an illusion as abstinence is ignored
"The United Nations Special Rapporteur on the right to health Mr. Pūras has called for "World needs "revolution" in mental health care". "There is now unequivocal evidence of the failures of a system that relies too heavily on the biomedical model of mental health services, including the front-line and excessive use of psychotropic medicines, and yet these models persist". Johannessen et al. 2021: "we must realize that today's drugs for the most serious mental disorders are not as effective as one might hope".
96 per cent of patients under compulsory mental health care received drug treatment (Bjerkan and Bjørngaard 2011). According to Leucht et al. 2017, 77% of patients are treatment-resistant non-responders, i.e. at least 70% of those forced drugged are medicated without benefit. It is both unreasonable and professionally indefensible, as the side effects are thus ignored and many patients' recovery is weakened in the long run.
Ranjan et al. 2025: Effectiveness of Psychological Intervention Methods: “Psychotherapies were found to be more effective compared to TAU”.
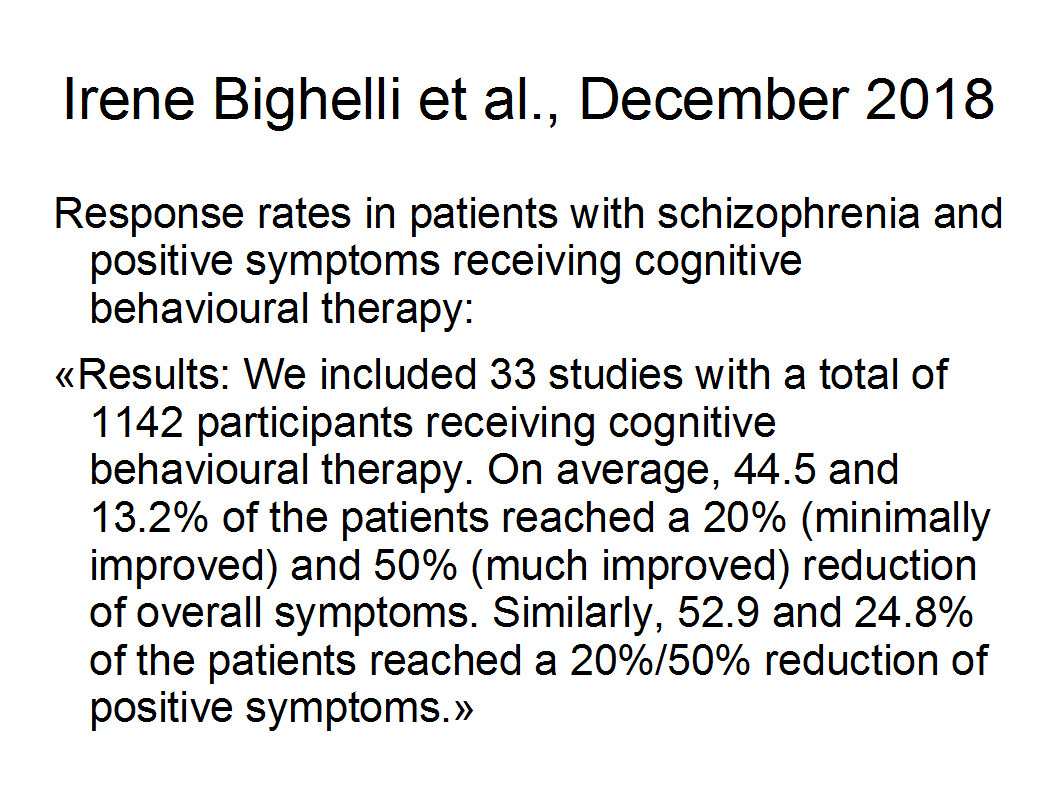
Cognitive Behavioral Therapy (CBT) was significantly superior to treatment as usual (TAU) for the outcome “overall symptoms”, “quality of life” and “functioning” (Bighelli et al. 2018) see WHO 2023 (mhGAP) guideline.
Because of. the patients' resistance, it is only with forced medication that so many can be medicated. The Civil Ombudsman found forced medication illegal on 21 January 2019 (statement 2017/3156), the Norwegian Directorate of Health has sabotaged the Civil Ombudsman by misinforming the State Administrator. After the Ministry of Health has also assessed that there is a "high probability" that healing will not be achieved, the Civil Ombudsman has again called for an end to forced medication on 5 November 2021. Both Norwegian National Human Rights Institution (NIM) and The Equality and Anti-Discrimination Ombud (LDO) are calling for an assessment of the knowledge base for forced medication in the light of human rights obligations.
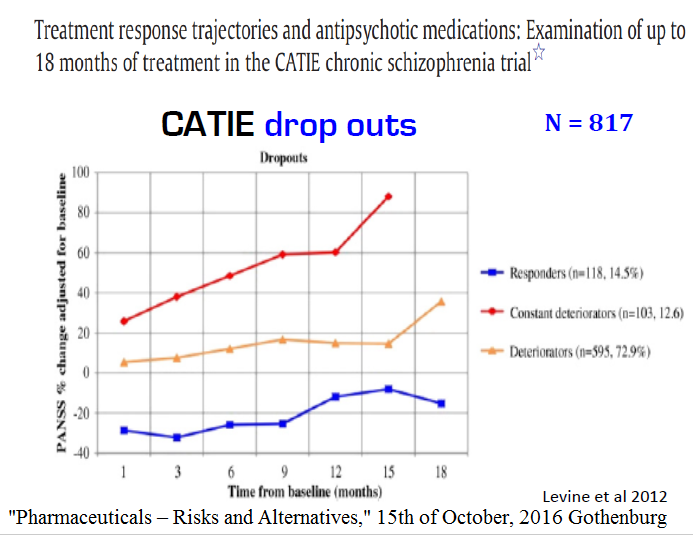
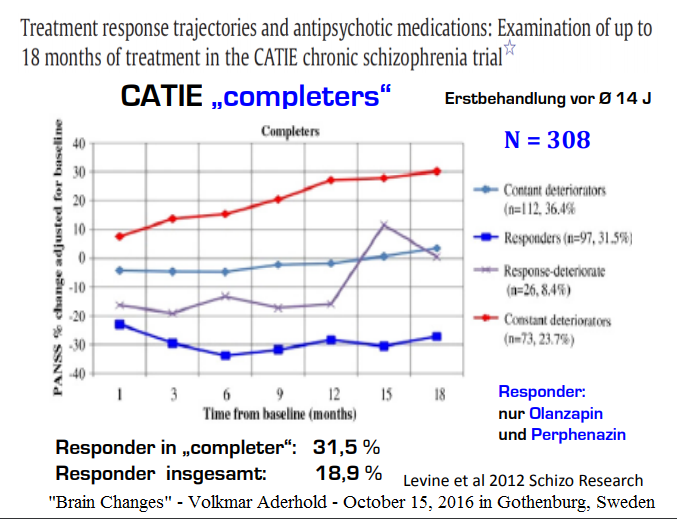
Due to little benefit and many side effects many patients want to stop taking antipsychotics (Lieberman et al. 2011: up to 74% drop outs) in 18 month CATIE study. The Tapering Anti-Psychotics and Evaluating Recovery (TAPER) Research Consortium is addressing this problem (Koops et al. 2023). HAMLETT is the abbreviation for “Handling Antipsychotic Medication Long-term Evaluation of Targeted Treatment”. Begemann et al. 2020 asked “To continue or not to continue? Antipsychotic medication maintenance versus dose-reduction/discontinuation in first episode psychosis. Results are scheduled for 2026 with study length 3.5 years. Antipsychotic Discontinuation and Reduction”. Study length is 2 years. (RADAR) showed showed that people who gradually reduce their antipsychotic medication are more likely to relapse than people who continue it. At 2-year follow-up there were no differences in social functioning, symptoms, side effects or quality of life.
Wunderink 2024: Antipsychotics Can Be Tapered Safely Without Increasing Relapse Risk. Tapering antipsychotics slowly and with supported decision-making may improve care for patients with psychosis. “Guided antipsychotic reduction to reach minimum effective dose in patients with remitted psychosis: a 2-year randomized controlled trial with a naturalistic cohort” (Liu et al. 2023) concluded: “Guided dose reduction group is a feasible approach as the majority of patients had a chance to taper antipsychotics to certain extents”.
On 10 June 2021, the WHO proposed coercion-free services such as Open dialogue, Basal exposure therapy and the Heidenheim clinic. Ending current treatment with forced medication promotes a paradigm shift from belief-based health-damaging overmedication to knowledge-based health-creating recommendations by the WHO and UN. Implementation of WHO's recommendations could possibly have the potential for 4 times as many patients to be treated.
Reference:
Paradigm Shift to Promote a Revolution of Treatment of Schizophrenia to Achieve Recovery. Walter Keim Dec 26, 2023. Medical Research Archives: https://esmed.org/MRA/mra/article/view/4866